
Clozapine Dose Adjuster Calculator
How Smoking Affects Your Clozapine
Cigarette smoke induces CYP1A2 enzyme, increasing clozapine metabolism. Smokers need 50-100% higher doses than non-smokers. When quitting, dose must be reduced by 25-30% to avoid toxicity.
Recommended Dose Adjustment
Monitor Blood Levels: Check weekly after changes
If you're taking clozapine and you smoke, your body is processing the drug differently than someone who doesn't smoke. It’s not just about habit-it’s about chemistry. Cigarette smoke triggers a powerful change in your liver that can make clozapine less effective, or worse, cause dangerous side effects if you quit suddenly. This isn’t theoretical. It’s happened to real people in hospitals, and it’s preventable.
Why Smoking Changes How Clozapine Works
Clozapine is a powerful antipsychotic used when other medications fail. It’s not like most drugs. About 90% of it is broken down by just one liver enzyme: CYP1A2. That’s unusual. Most drugs have multiple pathways to be cleared. Clozapine doesn’t. So when something boosts CYP1A2, clozapine gets cleared fast-too fast. Cigarette smoke contains chemicals called polycyclic aromatic hydrocarbons (PAHs). These aren’t just harmful to your lungs. They’re potent activators of CYP1A2. Within 24 to 48 hours of smoking, this enzyme starts working harder. After smoking about 20 cigarettes a day, CYP1A2 activity jumps by 2 to 3 times. That means clozapine disappears from your blood much faster. Studies show smokers need, on average, 50 to 100% more clozapine than non-smokers just to reach the same level in their blood. For example, a non-smoker might stay stable on 200 mg a day. A smoker might need 400 mg or more. If you don’t adjust for that, your symptoms could come back-hallucinations, paranoia, agitation. You might think the drug isn’t working. It’s not the drug. It’s your smoke.What Happens When You Quit Smoking
Quitting smoking is one of the best things you can do for your health. But if you’re on clozapine, quitting without a plan can be dangerous. When you stop smoking, CYP1A2 doesn’t shut off instantly. It takes about 38.6 hours for the enzyme activity to drop by half. After two days, it’s down 20%. By day 7, it’s down 36%. But your clozapine dose hasn’t changed. So now, the same amount of drug is building up in your system. Studies show that within two weeks of quitting, clozapine levels can rise by an average of 29.3%. That sounds small, but in clozapine’s world, it’s huge. The safe range is narrow: 350 to 500 ng/mL. Go above that, and you risk seizures, heart problems, or even life-threatening drops in white blood cells. One case report described a patient whose clozapine level jumped from 350 to 1,200 ng/mL after quitting smoking-over three times the upper limit. He ended up in intensive care. Clinicians have seen this pattern repeat. Reddit threads from psychiatrists report patients developing confusion, rapid heartbeat, and delirium after quitting smoking while on stable clozapine doses. The fix? Cut the dose by 25 to 30% right away. Then check blood levels weekly for the next two weeks. Don’t wait for symptoms. Don’t guess.Vaping Isn’t a Safe Alternative
Many people switch to vaping to quit smoking. But vaping isn’t a clean reset for clozapine. Traditional cigarettes burn tobacco, releasing PAHs that strongly induce CYP1A2. Vaping heats liquid without combustion, so it doesn’t produce the same level of these chemicals. That means CYP1A2 induction drops-sometimes sharply. One study found that switching from smoking to vaping led to clozapine levels rising enough to cause toxicity in some patients. But here’s the twist: some vape liquids contain aldehydes and carbonyls-chemicals that can still stimulate CYP1A2, just less predictably. So you might go from being over-dosed on clozapine because you smoked, to being under-dosed because you vaped, then suddenly overdosed when your body adjusts. It’s a rollercoaster. There’s no safe assumption here. If you switch from smoking to vaping, treat it like quitting smoking: monitor clozapine levels every week for two weeks. Adjust the dose based on blood tests, not guesses.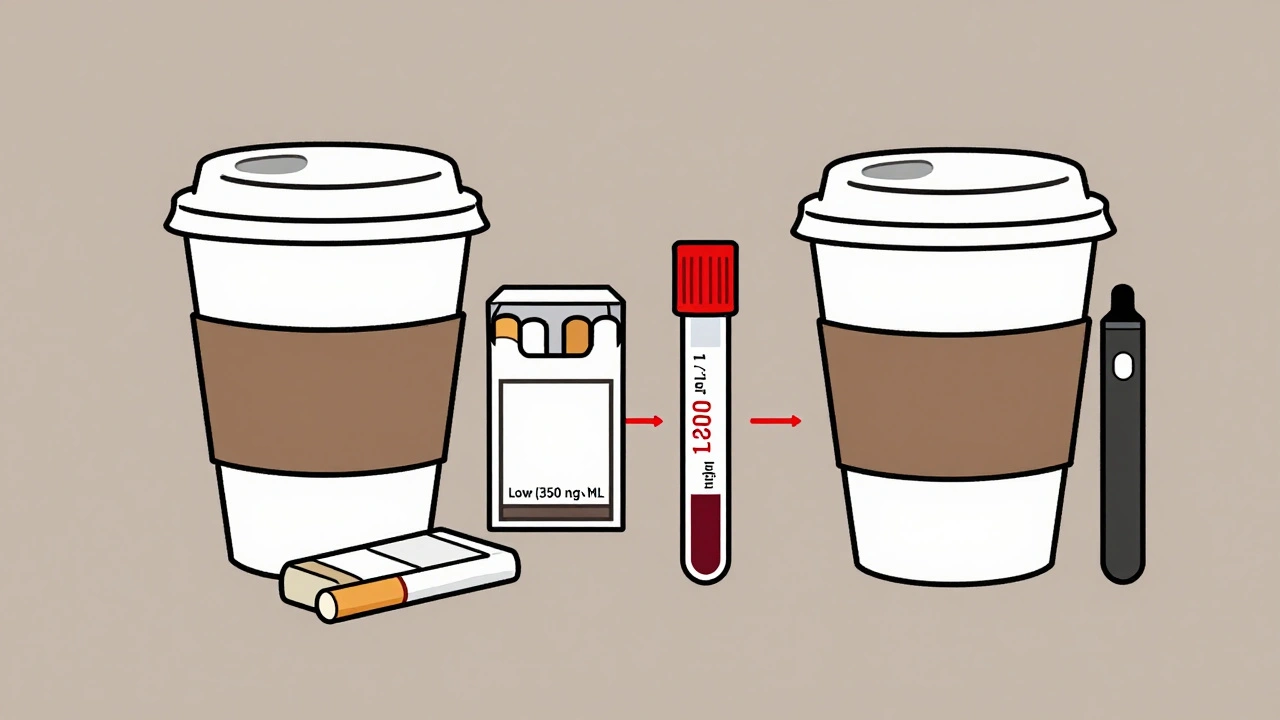
Genetics Don’t Override Behavior
You might wonder: does my DNA matter? Some people have a genetic variant called CYP1A2*1F that makes them more sensitive to enzyme induction. You’d think that would make a big difference. It doesn’t. A major 2003 study of 80 patients found no meaningful link between this gene and clozapine dose needs. Whether you have the variant or not, if you smoke, you need more drug. If you quit, you need less. Behavior wins over genes here. That’s good news in a way. You don’t need genetic testing to manage this. You just need to know your smoking status-and track your blood levels.Therapeutic Drug Monitoring Is Non-Negotiable
Clozapine isn’t a drug you take and forget. It requires regular blood tests. That’s not optional. It’s standard. The FDA has required therapeutic drug monitoring (TDM) since 2002. For smokers, the goal is to keep clozapine levels between 350 and 500 ng/mL. But because smokers clear the drug faster, their concentration-to-dose ratio (C/D) is much lower-usually below 0.8 (ng/mL per mg/day). Non-smokers? Their ratio is typically 1.5 to 2.0. If your doctor isn’t checking your levels every few weeks when you start clozapine-or every week after a change in smoking status-you’re not getting proper care. The Dutch Pharmacogenetics Working Group and the American Psychiatric Association both say: TDM is mandatory. And it’s not just about the dose. Timing matters. Blood tests should be done 12 hours after your last dose, at steady state-that’s about 10 days after any dose change. If you don’t wait that long, you’ll get misleading results.
What Happens If You Ignore This
Ignoring this interaction has real costs. People end up back in the hospital. A 2021 study found that improper dose management due to smoking changes led to 15-20% more hospital admissions. Each avoidable admission costs about $12,500. But the human cost is higher. One patient shared in a journal how, after quitting smoking, she went from 450 mg to 250 mg over 10 days with weekly blood tests. No side effects. No relapse. Just control. On the flip side, another patient, hospitalized for pneumonia, stopped smoking and didn’t adjust his dose. Ten days later, his clozapine level was 1,200 ng/mL. He had seizures. He needed ICU care. He survived. But he didn’t have to.What You Should Do Right Now
If you’re on clozapine and you smoke:- Don’t assume your dose is right. Ask for a blood test.
- If you’re planning to quit smoking, tell your doctor before you stop. Don’t wait.
- If you switch to vaping, treat it like quitting. Monitor levels weekly for two weeks.
- Ask about your C/D ratio. If it’s below 0.8 and you smoke, your dose is likely too low.
- If you quit smoking, expect to reduce your dose by 25-30% within the first week. Then check your levels.
What’s Next for Clozapine and Smoking
Researchers are working on better tools. One promising idea: a simple test using caffeine. Since caffeine is also broken down by CYP1A2, measuring how fast you clear it could tell doctors how active your enzyme is-without needing a clozapine blood test. Clinical trials are already underway. Another direction: new clozapine formulations that don’t rely so heavily on CYP1A2. That would make this whole issue easier to manage. For now, the solution is simple, but not easy: know your smoking status. Track your levels. Adjust your dose. Don’t let a habit-good or bad-put your treatment at risk.Managing clozapine with smoking isn’t about willpower. It’s about science. And science says: don’t guess. Test. Adjust. Repeat.













Eric Vlach
December 2, 2025 AT 10:30