When your neck starts to feel stiff and your hands seem to fumble more than usual-dropping keys, struggling with buttons, or tripping over flat ground-it’s not just aging. It could be cervical myelopathy, a serious condition where the spinal cord in your neck gets squeezed. This isn’t a vague discomfort. It’s a neurological problem that can quietly steal your coordination, balance, and independence if left unchecked. The most common cause? Cervical spinal stenosis-a narrowing of the spinal canal in your neck that presses on the spinal cord. Unlike simple neck pain, this is about damage to the spinal cord itself, and the effects can be permanent if not treated in time.
What Exactly Is Cervical Myelopathy?
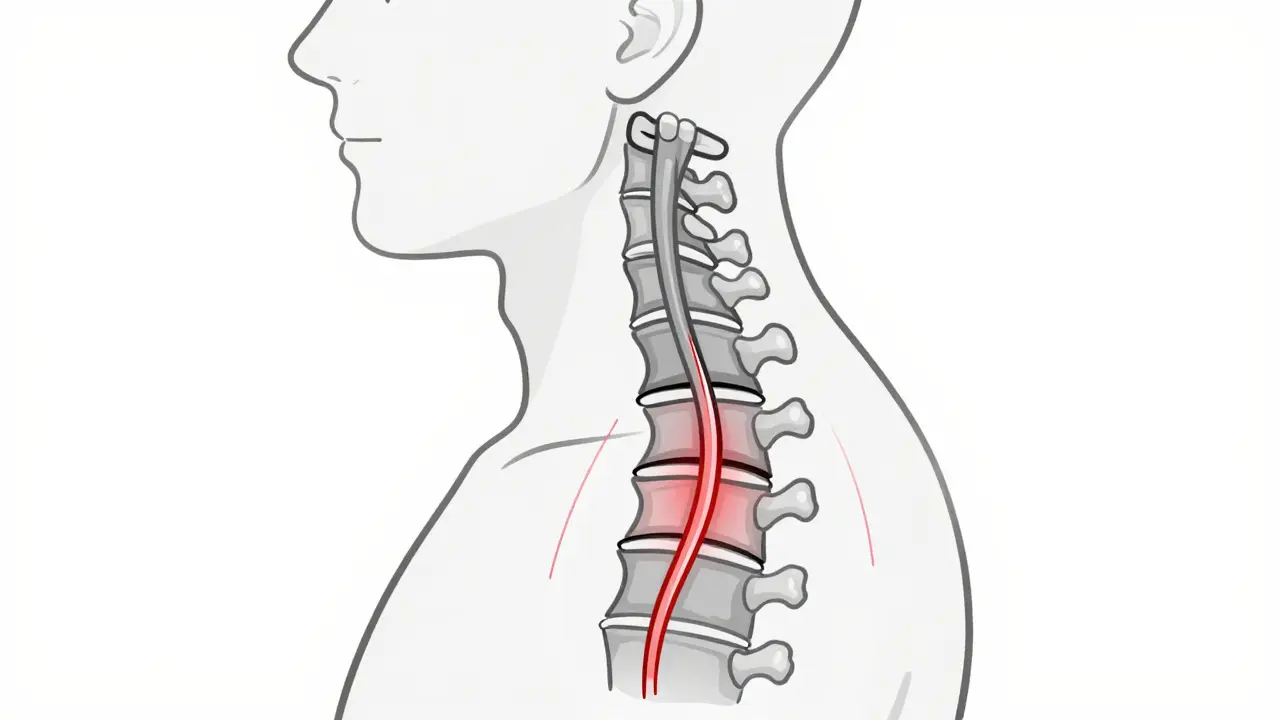
Cervical myelopathy isn’t just stenosis. Stenosis is the narrowing. Myelopathy is what happens when that narrowing damages the spinal cord. Think of it like a garden hose: if you step on it, water flow slows. If you crush it long enough, the hose gets damaged inside. That’s what happens to the spinal cord. The most common form is called cervical spondylotic myelopathy (CSM), which makes up about 75% of all cases in people over 55. It’s caused by years of wear and tear-discs flattening, bones growing spurs, ligaments thickening-all slowly closing in on the spinal cord.
Here’s what’s happening inside your neck: a healthy spinal canal is about 17-18mm wide. When it drops below 13mm, that’s stenosis. Below 10mm? Severe. That space gets taken up by bulging discs (which lose up to 30% of their height by age 60), enlarged facet joints, and thickened ligaments. The spinal cord doesn’t have room to breathe. And when it’s compressed, the signals from your brain to your arms and legs start to break down.
Early Signs You Can’t Ignore
The symptoms don’t always show up as neck pain. In fact, only about half of people with cervical myelopathy even have neck pain. The real red flags are subtle-and they sneak up slowly.
- Hand clumsiness: You drop things. You can’t button shirts. Writing becomes shaky.
- Gait instability: You feel unsteady walking. You bump into doorframes. You feel like you’re walking on cotton.
- Numbness or tingling: In your fingers, hands, or arms-not just when you sleep on them.
- Weakness: Your grip feels weaker. Your legs feel heavy.
- Balance issues: You need to hold onto walls or railings when walking.
- Bladder urgency: You feel the need to go more often, or you have accidents.
Neurologists look for reflex changes too. Overactive knee and ankle reflexes (hyperreflexia) are present in 85% of cases. If you’ve noticed any of these, especially if they’ve gotten worse over months, don’t wait. The Mayo Clinic found that 72% of patients with hand clumsiness and gait problems were diagnosed with myelopathy, not arthritis or nerve pinching.
How Doctors Diagnose It
There’s no blood test for this. Diagnosis needs two things: symptoms and proof of spinal cord compression. X-rays can show bone spurs and disc narrowing, but they don’t show the cord. That’s where MRI comes in. It’s the gold standard-97% accurate at detecting spinal cord compression. But it’s not just about the narrowing. The MRI must also show signal changes in the cord (T2 hyperintensity), meaning the cord itself is injured. Without that, you might just have stenosis without myelopathy.
Doctors also use the Japanese Orthopaedic Association (JOA) score. It’s a simple test that rates hand function, walking, bladder control, and sensation on a scale of 0-17. A score below 14 confirms myelopathy. EMG and nerve tests can catch early nerve damage even before symptoms are obvious. And here’s the kicker: up to 21% of people over 40 have stenosis on MRI with no symptoms at all. That’s why diagnosis isn’t just about the scan-it’s about matching the scan to your real-life problems.

When Surgery Becomes Necessary
Conservative treatment-physical therapy, NSAIDs, activity changes-works for a small group. About 28% of mild cases improve over two years. But 63% get worse. That’s why guidelines from the North American Spine Society and the American Academy of Orthopaedic Surgeons are clear: if you have moderate to severe myelopathy (JOA score under 12), surgery is the best option. Delaying it costs you recovery potential.
Studies show that patients who have surgery within six months of symptom onset recover 37% better than those who wait over a year. Dr. Wellington Hsu from Northwestern University says recovery drops by about 3% per month of delay. That’s not just a statistic-it’s your ability to hold a cup, walk without help, or stay independent.
Surgical Options: What’s Out There?
There’s no one-size-fits-all surgery. The approach depends on how many levels are affected, your spinal alignment, and your overall health.
Anterior approaches (from the front of the neck):
- ACDF (Anterior Cervical Discectomy and Fusion): Removes the damaged disc and fuses the bones. Works best for 1-2 levels. 85-90% of patients see neurological improvement. But 5-7% develop problems in nearby levels within 10 years.
- Cervical Disc Arthroplasty (Artificial Disc): Replaces the disc with a metal or plastic implant that keeps motion. Approved for multilevel use in 2023. In trials, 81% kept motion at 2 years vs. 63% with fusion. Less risk of adjacent segment disease.
Posterior approaches (from the back of the neck):
- Laminectomy: Removes the back part of the bone to open space. Good for multiple levels. But 18% of patients get chronic neck pain afterward.
- Laminoplasty: Hinges the bone open like a door. Preserves motion. Success rate of 82% for 3+ levels. Less neck pain than fusion, but slightly lower neurological recovery.
Combined approaches are used when the spine is unstable or curved abnormally. Surgeons now use robotic guidance and minimally invasive techniques like tubular laminoplasty, which cuts blood loss by 65% and hospital stays by nearly two days.
What Recovery Looks Like
Surgery isn’t a quick fix. You’re looking at 1-3 days in the hospital, then 3-6 months to return to normal activities. Most people need 8-12 weeks of physical therapy focused on balance, gait training, and strengthening neck muscles. About 82% of surgical patients report better hand function after a year. But only 65% fully regain stable walking. Some still need canes or walkers.
Complications happen. About 4-6% of patients have major issues: swallowing trouble (especially after anterior surgery), nerve injury (C5 palsy), or even worsening symptoms. That’s why choosing an experienced surgeon matters. Those who do over 50 cervical procedures a year have 32% fewer complications.
Why Timing Is Everything
Here’s the hard truth: once the spinal cord is permanently damaged, it doesn’t heal well. The damage isn’t always visible on scans until it’s too late. That’s why patients who wait too long often don’t get their full function back-even after successful surgery.
A Mayo Clinic study of over 1,200 patients found that those treated within six months were 2.7 times more likely to have “excellent” outcomes on the JOA scale. Those who waited over a year often had lasting weakness, poor balance, and bladder issues. The average time from first symptoms to diagnosis? 14.3 months. That’s more than a year of slow, silent damage.
What You Can Do Now
If you’re experiencing hand clumsiness, gait changes, or unexplained balance problems:
- See a spine specialist-not just a general doctor or chiropractor.
- Get an MRI within 2-4 weeks of symptom onset.
- Stop smoking. It doubles your risk of fusion failure.
- Control blood sugar if you’re diabetic. HbA1c below 7.0 cuts infection risk by more than half.
- Start gentle neck and core exercises. Don’t wait for surgery to stay strong.
And don’t downplay your symptoms. Many patients think it’s just arthritis or stress. But if your hands are losing dexterity or your walking is changing, this is neurological. It’s not something you can out-walk or out-sleep. It needs to be seen, diagnosed, and treated-before it’s too late.
What’s Next in Treatment
Research is moving fast. The FDA approved the first multilevel artificial disc in March 2023. Clinical trials are testing drugs like riluzole (used in ALS) to protect the spinal cord during surgery. Robotic-assisted surgery is on the horizon, with early data showing it could cut revision rates by nearly a third. But experts warn: we’re doing too many surgeries on people who don’t need them. Up to 20% of current procedures may be unnecessary. That’s why personalized treatment-using genetic markers and advanced imaging-is the future. The goal isn’t just to operate. It’s to operate at the right time, for the right person, with the right approach.
Can cervical myelopathy get better without surgery?
In mild cases with stable symptoms, some people improve with physical therapy and activity changes-but only about 28% do. The majority (63%) continue to decline. If symptoms are getting worse, especially with hand clumsiness or walking problems, surgery is the only way to stop progression and restore function. Waiting doesn’t help-it makes recovery harder.
How do I know if my neck pain is just soreness or cervical myelopathy?
Neck pain alone isn’t a sign of myelopathy. The red flags are neurological: trouble with fine motor skills (buttoning shirts, writing), unsteady walking, frequent tripping, numbness in hands, or bladder urgency. If you have these, even without severe pain, you need an MRI. Many patients with myelopathy have little to no neck pain.
Is cervical disc replacement better than fusion?
For single-level disease, both work well. Disc replacement preserves motion and reduces the risk of problems in nearby levels. Fusion is more predictable for older patients or those with instability. Newer artificial discs approved in 2023 now work for two or three levels, making them a strong option for many. But not everyone is a candidate. Your spine alignment, bone quality, and number of affected levels determine the best choice.
How long does recovery take after cervical myelopathy surgery?
Hospital stay is usually 1-3 days. You’ll need 6-12 weeks of physical therapy. Full recovery-returning to normal activities, strength, and balance-takes 3-6 months. Hand function often improves within 3-6 months. Walking stability can take longer, and some people still need a cane. Patience and consistent rehab are key.
What happens if I ignore my symptoms?
Untreated cervical myelopathy leads to irreversible damage. Studies show 20-60% of untreated patients worsen over 2-5 years. You could lose the ability to walk, grip objects, or control your bladder. In severe cases, paralysis below the neck is possible. Early surgery stops progression. Delaying it doesn’t give you time to heal-it gives the damage time to spread.








Nilesh Khedekar
March 17, 2026 AT 19:32